
The Basic Healthcare Provision Fund (BHCPF), a Federal Government initiative targeted at easing access to healthcare for the most vulnerable Nigerians, is revolutionising healthcare access in some rural areas of Niger State, by addressing critical issues such as decaying facilities, drug and staff shortages in health centres. Hamzat Ibrahim Abaga explores the positive changes observed during his visit to health centres in Agaie, Bosso and Lapai local government areas.
Before the introduction of the Basic Health Care Provision Fund (BHCPF), a Federal Government initiative aimed at providing accessible and affordable healthcare services to vulnerable Nigerians in 2021, the Comprehensive Primary Healthcare Centre, (PHC) in Etsugaie, Agaie Local Government Area (LGA), was a symbol of decay, with dilapidated infrastructure, insufficient supplies, and inadequate human resources.
But with the intervention, the once struggling facility undergone a total renovation, leading to an improvement in medical services and the availability of essential items like drugs.
For the community members, this transformation was not just a cosmetic change but a crucial restoration of access to quality healthcare.
Muhammad Ndagi, the Officer-in-Charge (OIC) of the PHC, reminisced on the past difficulties the facilities faced, saying, “they [patients] would come for treatment, but there would be no necessary items in the clinic.”
Today, the centre has been revitalised and community trust in the healthcare system has been restored.
“We didn’t even have mattresses in the clinic in the past, until we started receiving BHCPF funds and we replaced them all,” Ndagi said.
Zainab Ibrahim, a member of the Ward Development Committee (WDC), corroborated Ndagi’s claims, saying that “unlike the previous years, there are now drugs at the centre.”
Access to essential medications is crucial for improving health outcomes and reducing mortality rates. The revitalisation of PHC Etsugaie has provided a lifeline to the local community, ensuring that healthcare is both accessible and reliable.
This centre is among over 200 facilities in Niger State benefiting from the federal government’s health intervention programme.
Virtually all the focal PHCs across Niger State assessing the BHCPF have been renovated, wearing a combination of blue and milk-coloured exteriors.
When this reporter visited the Etsugaie PHC and Beji PHC in Bosso amd Agaie LGAs in Niger State, he observed that facilities have been revamped, each with new ceilings, roofing, motorised boreholes, and extensions of new buildings.
Staff at the facilities said they had delivered their service inside unconducive buildings with inadequate amenities.
THE BIRTH OF BASIC HEALTHCARE PROVISION FUND (BHCPF)
The BHCPF is established under Section 11 of the National Health Act (NHA Act), 2014, as the principal funding vehicle for the Basic Minimum Package of Health Services (BMPHS).
The Fund serves to increase the fiscal space and overall financing to the health sector to assist Nigeria, particularly the most vulnerable – women, children, the elderly and People With Disability (PWDs), achieve Universal Health Coverage (UHC).
Funding of the BHCPF is derived from contributions including an annual grant from the Federal Government of Nigeria of not less than 1% of its Consolidated Revenue Fund (CRF), grants from international donor partners and funds from any other source.
The National Primary Health Care Development Agency (NPHCDA), which oversees the scheme, states that the BHCPF aims to achieve Universal Health Coverage (UHC), with targets of 30 percent coverage in three years, 70 percent in five years, and full coverage in seven years.
READ ALSO:
- Understanding Sleep Paralysis: A Terrifying Experience of Feeling Dead
- The Impact of AI on Healthcare: Transforming Patient Care
- How Mental Health Impacts Physical Well-being
The BHCPF also aims to ensure that each of Nigeria’s 774 LGA has at least one functional public or private primary health care facility.
These centres are essential for handling short-term and uncomplicated health issues, but many of them have faced neglect and a lack of qualified personnel.
The federal government said it has disbursed a total of N103,541,090,666 for the BHCPF since the commencement of its implementation in the country. The Coordinating Minister of Health and Social Welfare, Professor Muhammad Ali Pate, disclosed this during the Ministerial Oversight Committee meeting on the BHCPF in April this year.
RECRUITING STAFF WITH BHCP FUND
Since receiving BHCPF funds since January this year, Halima Musa, OIC of Beji Primary Health Centre (PHC), has employed a nurse and a private security guard to assist with the day-to-day management of the facility.
She stated that the centre operates with 22 permanent staff members and many students.
“The last time we received BHCPF funds was in January 2024, and we received N300,000,” she said.
She noted that the facility started benefitting from the BHCPF in 2022, receiving N300,000 every quarter. The money, she said, has been used for overall repair and maintenance of the facility.
 Musa explained that hiring a private security guard and a casual nurse was essential to maintain the facility’s security and ensure coverage during her absences or night shifts. Both the security guard and the casual nurse are paid a monthly stipend of N15,000 each from the BHCPF fund.
Musa explained that hiring a private security guard and a casual nurse was essential to maintain the facility’s security and ensure coverage during her absences or night shifts. Both the security guard and the casual nurse are paid a monthly stipend of N15,000 each from the BHCPF fund.
“We pay both the security and casual nurse N15,000 from the BHCPF fund and also with a monthly allowance,” Musa added.
“I decided to hire casual staff to prevent the facility from deteriorating, as many of the 22 permanent staff members are not always available.”
Similarly, in Etsugaie, OIC Ndagi confirmed that part of the fund is used to employ a midwife and a private security guard.
“We have two staff (a private security guard and a midwife) under our facility, paying them N7,000 and N10,000 monthly,” said Ndagi.
BHCPF FUNDS HELP BEJI PHC STAFF AND IMPROVE SERVICE DELIVERY
Speaking to the casual staff at Beji PHC, 24-year-old Sumaiya Yusuf, she explained that her initial plan was to return to her tailoring apprenticeship after graduating from school.
She was not expecting to get a job soon in a country where graduates are jobless. However, she was fortunate to be retained as a casual staff member, where she completed her one-year industrial attachment and received accommodation at the PHC staff quarters.

Sumaiya noted that her time at the facility had significantly contributed to her professional development, as she was involved in practical tasks every day.
“It has helped me a lot,” she said. She elaborated, “Initially my plan was to return to my tailoring apprenticeship after graduating from school.
“I never expected to easily find work due to the scarcity of jobs in Nigeria. However, I was fortunate enough to be retained as a casual staff member, where I completed my one-year industrial attachment and even had accommodation at the PHC staff quarters.”
However, she also highlighted the difficulties she faced when commuting from Maikunkele, the headquarters of Bosso LG, to Beji, often spending more on transportation than she earned.
“Every day I spent N1,200 and when the price got almost N1,600, I found it difficult to go.” Sumaiya’s engagement has allowed Beji PHC to provide 24-hour service delivery, according to Musa.
THE BHCPF AND ITS ROLE IN NIGERIA’S HEALTH SECTOR REFORM PROCESS
In Nigeria’s healthcare system, multiple agents operate at different levels, influencing how services are delivered. The government plays a central role, supported by two key technical agencies: the National Primary Health Care Development Agency (NPHCDA) and the National Health Insurance Scheme (NHIS).
These bodies are responsible for healthcare delivery, but private providers dominate in many areas, serving about 60% of the population (Alliance for HPSR and WHO, 2017).
Data from the 2018 Demographic and Health Survey (DHS) indicates that 46.5% of Nigerians seek treatment from private chemists and patent medicine vendors for childhood fevers, while 18.1% visit government health centres (NPCN and ICF, 2019).
Health Maintenance Organizations (HMOs) also play a key role in Nigeria’s healthcare system. HMOs were introduced in the mid-1990s, modeled after the U.S. ‘managed care’ system, and initially provided private health insurance for firms (Onoka et al., 2015). When the NHIS was established in 1999, HMOs became operators of the scheme, offering insurance plans and managing healthcare provider networks (Onoka et al., 2016).
The private sector’s dominance in healthcare is tied to the underfunding of public health services over several decades. To address this, the Basic Health Care Provision Fund (BHCPF) was established in 2018, offering an additional funding stream for healthcare.
READ ALSO:
- History of Primary Education in Nigeria
- The Benefits of Journaling for a Healthier Lifestyle
- 25 Health Benefits Of Bitter Leaf
The ‘Guideline for the Administration, Disbursement and Monitoring of the Basic Health Care Provision Fund’ (2020 Guidelines) guides its implementation (FMOH, 2020). The BHCPF operates through three ‘implementation gateways’:
The first, the NHIS gateway directs 50% of BHCPF resources to State Health Insurance Schemes (SHISs), which use the funds to provide a Basic Minimum Package of Health Services (BMPHS) at eligible primary and secondary healthcare facilities.
The second, the NPHCDA gateway allocates 45% of the BHCPF to public primary healthcare facilities to support drug procurement, facility maintenance, equipment purchase, and staff investment, ensuring that at least one functional primary healthcare facility exists in each political ward (NPHCDA, 2018).
The final 5% is reserved for emergency medical treatment (EMT gateway).
THE FACE OF BEJI AND ETSUGAIE PHC BEFORE THE INTERVENTION OF BHCPF
Musa, the OIC of Beji PHC, recalled when she was posted to the facility in 2015. According to her, there was no power supply. Through the Basic Health Care Provision Fund (BHCPF), she was able to connect the facility to electricity. Built in 1993, Beji PHC serves the village and 28 surrounding communities.
It was reconstructed in 2016 by the state government. The facility includes a solar-powered water borehole, an eight-room staff quarters and a fully equipped laboratory, all provided through BHCPF.
“When I was first posted here in 2015, the facility didn’t have access to power supply, and through money from BHCPF, I was able to connect electricity. Also, due to the engagement of casual staff and security guards, the facility now operates 24 hours a day,” Musa stated.
In Etsugaie PHC, Ndagi, the OIC, explained that BHCPF funds were used to provide potable water, mattresses, beds, solar panels, and free patients’ cards as motivation for clinic visits. These were all done over time, he said.
WDC, PHC COLLABORATION DRIVING POSITIVE CHANGE
Beji PHC stands out from other beneficiaries of the BHCPF in the state due to the collaboration between the Ward Development Committee (WDC) members and the facility’s management.
“Whenever the BHCPF funds are released, the management of Beji PHC immediately informs the Ward Development Committee (WDC),” Musa explained.
Significantly, this is the working relationship envisaged in creating WDCs usually made up of leaders in the community where a PHC is cited. This collaboration enables all stakeholders to be involved in the decision-making process and brings about transparency and accountability.
“We call a meeting to discuss and deliberate on the needs of the facility. This is to ensure that the funds are used to address the most urgent priorities,” she added.
Musa noted that this inclusive system has improved the facility’s operations and strengthened trust between the staff and the community.
“It’s a partnership that works for the benefit of everyone,” she said. Beji PHC has become a model in the region, delivering improved services and gaining widespread recognition.
“Through WDC, the PHC has annual, quarterly, and immediate development plans. These are plans to keep the activities of the facility running on a daily basis,” Musa explained.
Baduku Aminu Ahmed, Chairman of Beji WDC, confirmed this, adding that BHCPF funds are used effectively through mutual collaboration.
“We convene a meeting to evaluate and address the facility’s needs,” Ahmed said.
In Etsugaie PHC, Abdullahi Jibrin, Secretary of WDC, noted that regular meetings with PHC staff have led to decisions such as subsidising drugs and using funds for volunteer payments.
Ndagi, the OIC of Etsugaie PHC, corroborated him, saying, that “whenever the fund comes, we meet with WDC members to decide how the money should be used.”
ETSUGAIE, BEJI PHC SEEKS GOVERNMENT INTERVENTION FOR STAFFING
Despite these improvements, Etsugaie PHC faces a critical manpower crisis, with only two Community Health Extension Workers (CHEWs) available, risking the facility’s closure if these staff members are absent.
“Etsugaie PHC urgently needs additional nurses and midwives to handle deliveries and other essential tasks,” Ndagi, the OIC of Etsugaie, noted.
“Lack of adequate manpower is our major problem. We only have two CHEWs, and if they are not around, the facility will be closed. We need the government to come to our aid by providing more staff for us. We need nurses and midwives.”
Meanwhile, Musa, the OIC of Beji PHC, also expressed frustration over the severe shortage of human resources at her facility.
He added that previous appeals to the Director of PHCs at Bosso LGA and Bosso local government authorities have not yielded any results.
She also observed that the N300,000 quarterly fund provided to her is insufficient to meet her needs, stating that “the amount is not enough to cover the basic requirements, let alone additional expenses.'”
“I will love it if we can get a medical doctor and enough nurses in the facility to render effective services to the community. We also need an ambulance,” Musa said.
NEGLECT AT CHEKU AND DUMA PHCS AS BEJI AND ETSUGAIE THRIVE
While residents of Beji and Etsugaie benefit from standard primary healthcare services, residents of many other communities, including Cheku and Duma, both of Lapai LGA, feel neglected by the government.
Farook Ndako, the OIC of Duma PHC, highlighted severe challenges faced by the facility. Despite receiving money for medications and supplies, the building is in poor condition.
“The physical structure is over fifty years old and no longer habitable. It desperately needs expansion,” Ndako said.
The facility has seven staff members – three male and four female nurses -but Ndako emphasised this is insufficient given the growing population.
“We have reported these challenges to local government officials, who have escalated them to the state, but we are still awaiting a response,” Ndako added.
A visit to Cheku PHC revealed similar issues with the facility’s condition and staffing.
Umar Adamu, the OIC, said, “We operate with just one permanent staff and rely on volunteers to manage healthcare for 14 communities, including people from Edo, Yelwa, and Bina.”
The facility suffers from a lack of reliable water and inadequate bed space among others.
“The ceiling is badly damaged, leading to infestations of beds and other areas by animals, which makes it extremely difficult for both staff and patients to cope,” Adamu said.
274 PHCs BENEFITS FROM BHCPF – SHOW IMPROVED PERFORMANCE
In response to a Freedom of Information Act (FOIA) request, the Niger State Ministry of Primary Health Care (MPHC) said that 274 healthcare centers across the state have benefited from the Basic Health Care Provision Fund (BHCPF).
In the ministry’s response signed by Dr. Abdullahi Usman Imam, the Permanent Secretary of the ministry, it disclosed that the state received N495,289,476.15 in 2020, no allocation in 2021, N297,625,200.65 in 2022, N716,222,739.24 in 2023, and N343,360,485.48 in 2024 under the BHCPF initiative, all amounting to N1, 852,497,901.52.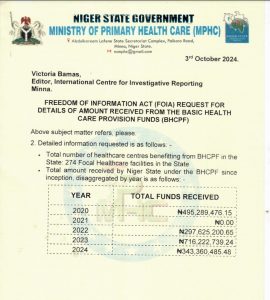
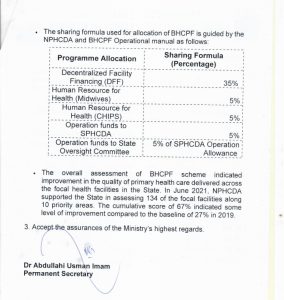 The ministry also noted that the distribution of these funds follows the guidelines set by the National Primary Health Care Development Agency (NPHCDA) and the BHCPF Operational Manual.
The ministry also noted that the distribution of these funds follows the guidelines set by the National Primary Health Care Development Agency (NPHCDA) and the BHCPF Operational Manual.
In the allocation formula:
35% of the funds go to Decentralized Facility Financing (DFF),
5% to Human Resources for Health (Midwives),
5% to Human Resources for Health (Community Health Influencers, Promoters and Services, or CHIPS),
5% to operational funds for the State Primary Health Care Development Agency (SPHCDA), and another
5% to the State Oversight Committee as part of the SPHCDA operational allowance.
The FOIA response highlighted that the BHCPF has contributed to significant improvements in healthcare delivery in the state. It also referenced a performance assessment supported by the NPHCDA in June 2021, where 134 focal facilities were evaluated across 10 priority areas.
In effect, the cumulative score from the assessment was 67%, a considerable increase from the baseline score of 27% recorded in 2019.
The document noted that this positive shift in performance is a proof of the overall impact of the BHCPF on strengthening primary healthcare services across Niger State.
FOMWAN SUGGESTS STRATEGIES FOR EFFECTIVE UTILISATION OF THE BASIC HEALTHCARE PROVISION FUND
Hajiya Hauwa Kulu, Amira of the Federation of Muslim Women Association of Nigeria (FOMWAN) Niger State chapter, called for better management of the BHCPF by PHC managers.
Kulu stated that the purpose of BHCPF is to cover operational costs and provide necessary supplies, and thus the importance of accountability and collaboration with Ward Development Committees (WDCs) should be highlighted.
To maximise the fund’s impact, Kulu advocates for transparency in financial transactions.
“Every kobo must be accounted for,” she says, emphasising that “community trust is dependent on transparent financial management. Involving WDCs in fund monitoring can improve accountability and increase local engagement.”
She also recommends strategic planning as a key approach. Before disbursing funds to PHCs, state and local governments should establish clear budgetary allocations so that everyone involved understands the financial framework.
Furthermore, she said that collaboration with local philanthropists can help supplement funding and improve facility maintenance. By effectively utilising the BHCPF, she noted, PHCs can significantly improve maternal healthcare services, benefiting the entire community.
Kulu further emphasised the importance of strategic measures in PHC’s to maximise the impact of the BHCPF in the State.
She noted that these measures should emphasised effective feedback and monitoring.
Kulu advocates for increasing the capacity of WDCs, stating, “By empowering these committees, they can effectively monitor fund expenditures within their jurisdiction, assisting in identifying and addressing any financial leakages.” This oversight will make it easier to reinvest recovered funds into facilities that need to be improved.
She also emphasised the importance of creating a feedback platform for citizens to share their experiences with healthcare services. “This feedback mechanism will allow for continuous assessment and improvement of health services, ensuring that BHCPF meets its goal of improving healthcare delivery in rural areas,” Kulu concluded.
On his part, Mathew Oladele, the Programme Director of the Initiative for Social Development in Africa, iSODAF, an initiative that promotes social accountability by using public data to advocate for improvements in healthcare and education services, said that to enhance the effectiveness of the Fund, it is essential to streamline the allocation directly to healthcare facility managers, bypassing state government bureaucracy.
Oladele also advocated for critical reforms, emphasising the importance of community-based organisation representatives overseeing fund management.
“When this is done, communities will have more confidence in the system.”
Furthermore, establishing the BHCPF account as a community-based funding mechanism would enable local members to contribute to the fund, he opined.
“This will make the program more efficient and sustainable,” Oladele explained.
Integrating town hall meetings with community members into the needs assessment report would also be beneficial, he noted, while recommending the alignment of basket funding, including which includes both BHCPF and community contributions, and the prioritisation of essential services to better serve citizens.
Oladele further stated that the community members should be empowered to address infrastructure challenges directly, adding that “the government should not come awarding contracts with BHCPF funding.”
This report was done with the support of the International Centre for Investigative Reporting, ICIR.